Introduction
Resorption of mandibular ridge is a multifactorial and biomechanical disease that is chronic, progressive, irreversible, and cumulative leading to loss of sulcular depth, vertical dimension loss, and decreased lower facial height. The denture becomes passive due to complex neuromuscular control and causes difficulties in impression-making, mastication, and swallowing, which in turn leads to loss of retention and stability in complete dentures.1 Therefore, it becomes difficult for the dentist to fabricate a denture in such situation. To increase the stability and retention of mandibular denture, previous reports have recommended that posterior denture teeth be positioned directly over the crest of the edentulous ridge.
This relationship of the teeth and alveolar ridge is important for the stability of the denture in function. Although this tooth position may be desirable when adequate alveolar ridge height is available, such a position may not be suitable for severely resorbed ridges because of a lateral shift in the orientation of the ridge crest.
This horizontal discrepancy between original tooth position and resorbed ridge crest, coupled with an increased vertical distance between occlusal table and tissue support, can lead to denture instability.
Successful denture treatment in situations like this can become increasingly dependent on the position of the denture teeth and the external contours of the dentures.
It is for these patients that the neutral zone concept becomes increasingly significant. The lower denture commonly presents the most difficulties with pain and looseness being the most common complaint. This is because the mandible atrophies at a greater rate than the maxilla and has less residual ridge for retention and support.
The neutral zone technique is most effective for patients who have had numerous unstable, unretentive lower complete dentures. These patients usually have a highly atrophic mandible and there has been difficulty in positioning the teeth to produce a stable denture.
Fish, in 1931, first described the influence of the polished surfaces on retention and stability. He also described how dentures should be constructed in the ‘dead space’, which later came to be known as the neutral zone.2
The neutral zone has been defined as the potential space between the lips and cheeks on one side and the tongue on the other; that area or position where the forces between the tongue and cheeks or lips are equal.3
The purpose of this article is to present three cases with resorbed ridges treated with the neutral zone technique for the fabrication of successful and stable mandibular complete denture with severely resorbed ridge.
Case Report 1
A 70 years –old- male patient came to the OPD in the department of prosthodontics with history of previous denture and having the chief complaint of very loose mandibular complete denture. Figure 1

Technique
The primary impressions were made in stock tray with a mucocompressive material, impression compound. The acrylic special tray was fabricated for the secondary impression. Figure 2
The maxillary secondary impression was made in special tray with low fusing impression compound and zinc-oxide-eugenol material.
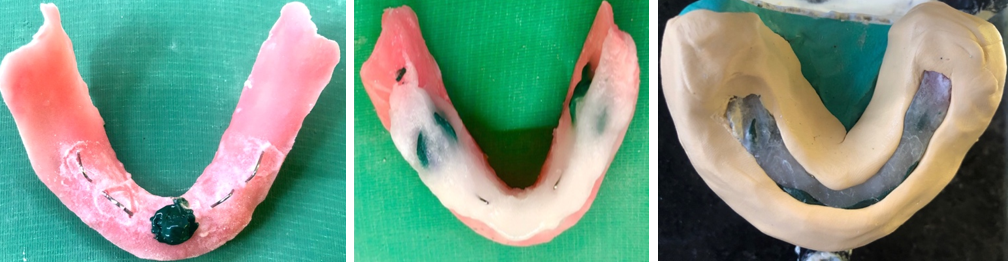
The mandibular secondary impression was made in admix technique, It's a combination of impression compound and green stick (low-fusing) compound in the ratio of 3:7. Figure 3
The occlusal rims were made on heat cured acrylic denture bases.
Mandibular occlusal rim was completely removed and wire loops were attached over the record base in accordance with recorded vertical height. 4
The impression compound and green stick in ratio 3:7 was softened in a 65 degree C water bath. Figure 4
The softened compound was kneaded and a roll was formed according to the crest of the ridge and was adapted to the retentive loop at established vertical dimension.
The attached roll of compound was reheated in the water bath, with the record base firmly seated, the patient was asked to perform a series of functional movements like swallowing, speaking, sucking, pursing lips, pronouncing vowels sipping water and slightly protruding the tongue several times which simulated physiological functioning. These actions will mould the material by muscle activity.
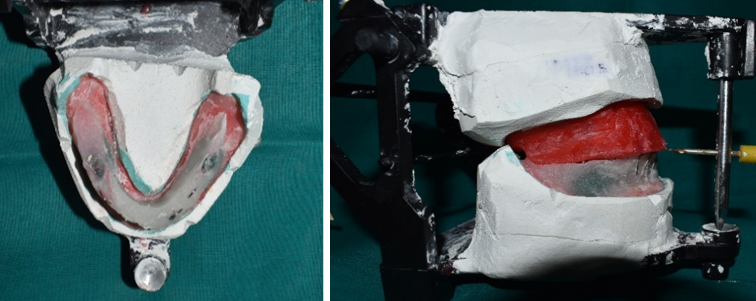
After 12 minutes approximately it was removed from the patient’s mouth. Neutral zone impression which was made was transferred to the master cast, the grooves were cut on the master cast and a silicone putty index was made around it.Figure 5
The neutral zone impression compound was removed, replaced by modelling wax and then teeth arrangement was done exactly following the putty index. Figure 6
After the teeth arrangement try in was done of the waxed-up dentures in the patient’s mouth, after which the patient was asked to repeat all the functional movements. This was done to confirm the stability of the denture during all the border movements. The dentures were then processed in a conventional manner.
The dentures were finished and polished in order to maintain the contour of the polished surfaces. Figure 7






Case Report 2
A 68-year-old male completely edentulous patient reported to the Department of Prosthodontics, with the chief complaint of difficulty in chewing due to missing teeth. On examination, it was found the mandibular ridge was extensively resorbed (ATWOOD ORDER-5). The treatment plan decided for this patient was a conventional maxillary complete denture and a mandibular complete denture fabricated by neutral zone technique.Figure 8

Technique
The Preliminary impression, secondary impression, Jaw relations was recorded in conventional manner.
The mandibular wax rim was replaced with four wire stoppers and one central stopper made of low fusing impression compound. The tissue conditioner was placed on the altered record base.5 The patient was instructed to speak, swallow, drink some water several times to mould buccal and lingual surfaces of the tissue conditioner.Figure 9
The lower record base was placed back on the mandibular cast. A Putty index was made around neutral zone.
Modelling wax was flowed according to the putty index and the teeth were placed according to that. Firstly the lower teeth were placed and checked according to the putty index, the maxillary teeth were arranged according to the location of mandibular teeth.
Try-in of waxed denture was carried out evaluating aesthetics, functions and patient satisfaction.
The maxillary and mandibular dentures were processed in conventional manner and insertion was done.Figure 10

Case Report 3
A 72-year-old male patient reported to the Department of Prosthodontics with a chief complaint of an old unstable mandibular complete denture. The patient was advised for the fabrication of complete denture with neutral zone technique as other treatment options like implant-supported complete dentures was not feasible due to the age and cost factors.
The lower ridge was having ATWOOD ORDER-5. The primary impression was made using Irreversible Hydrocolloid impression material with a perforated edentulous stock tray. Closely fitting custom tray was fabricated and the border moulding was performed with low fusing impression compound (green stick) and Impression compound (Admix technique) to represent muscle activity, thus recording the functional depth and width of the sulcus. The final wash impressions were made with Zinc Oxide Eugenol impression paste.
Procedure
After examination, the previous dentures were found to be unstable and non-retentive and could not be relined.
After adequate impression making, master cast was poured in dental stone.
The wax record rims were fabricated and assessed for appropriate extensions.
Jaw relation was done and vertical and centric relation was recorded and mounting was done on an articulator.
Another set of denture bases were fabricated on the duplicated master cast.
The mandibular rim was made to match the same vertical height with maxillary rim thus, maintaining the vertical stop.
Now, to record the neutral zone the patient was asked to sit in an ustrained, upright position and the head not supported.
The mandibular denture base, along with Tissue Conditioner was inserted into patient’s mouth and the patient was asked to smile, grin, purse his lips, and count from 60 onward, loudly, he was made to pronounce the vowels, sip water, swallow, was asked to protrude the tongue and licking of lips. Following actions were continued for 10 minutes until the Tissue Conditioner hardened.
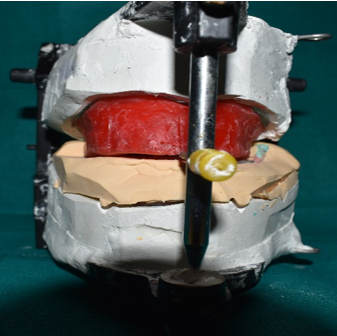
The Tissue Conditioner rim was placed on the second ie, duplicated master cast. The putty index was made around the Tissue Conditioner rim.Figure 11
Then the Tissue Conditioner rim was removed from the denture base and the index was placed over the cast. The index preserved the space of the recorded neutral zone. 6
Modelling wax was poured into the putty space to reproduce the neutral zone. Figure 12
The new wax rims were then placed again on the casts on articulator.
Teeth arrangement was carried in the neutral zone space (putty index).
The position of teeth was checked by placing the indices around the arranged teeth.
Try-in was carried out.Figure 13
Dentures were flasked, cured and finished in a conventional way, preserving the flange contours.
Dentures were finally checked for any sharp points and inserted.

Discussion
The muscle movement around the denture is dynamic. The records obtained from neutral zone technique are patient specific yet it is reproducible in position, width and shape. The conditions which influence the neutral zone records are numerous, such as functional movements, materials used to record, technique used, muscle tone, vertical dimensions, the period of complete edentulism, etc. Since many years, researchers have been exploring the appropriate tooth position for complete dentures.7
Denture constructed over a highly resorbed mandibular ridge, using neutral zone technique distributes the muscular forces and enhances the retention and stability of the denture, thus inhibits dislodgement of denture while in function. The dentures thus constructed, are superior in design, as there will be reduced food lodgement, with better esthetics, adequate placement of the posterior teeth which permits sufficient tongue space.
The material commonly used in the study was- low fusing impression compound and tissue conditioners. The ideal material used to record the neutral zone should have following properties – it should be soft, should have enough working time and should mould according to the tongue movements and circumoral musculature, thus accurately record the neutral zone. The materials used in the present study were the combination of geen stick, impression compound (admix) and tissue conditioner.
Admix material was used to record the neutral zone, it combines Impression compound and Green stick (low-fusing) compound in 3:7 ratio. The Low-fusing compound when mixed with the impression compound, forms a low viscosity material, which is easy to manipulate according to the oral musculature. The admix material has a better flow and results in an accurate impression
Tissue conditioners are visco-elastic materials, they express varied degree of plastic flow for more than 24 hours after the mixing. The process by which they undergo a transition from a fluid mass to a viscous, flexible, sponge-like thick solid is based on gelation. These materials have extended working time, they flow for a longer duration and also they do not resist the forces exerted by the surrounding tissues and have higher flow rates, even after 24 hours.8
Conclusion
Since the 1930’s the neutral zone concept has been practiced by several prosthodontists. It is one of the best alternative techniques for atrophied mandibular ridges, but it is not very commonly used because of the extra clinical step involved, additional lab costs, increased chair time and complexity. It is very useful in cases where dental implants are contra-indicated. The main motive of establishing the neutral zone is to fabricate a denture which has a good muscular equilibrium, as the main factor in the denture retention and stabilization in the patient with resorbed ridges is the muscular control and balance during function.