- Visibility 287 Views
- Downloads 21 Downloads
- DOI 10.18231/j.jds.2020.019
-
CrossMark

Management of calcified canal in the traumatised maxillary central incisor using magnification
Introduction
Dental pulp obliteration is also called as calcific metamorphosis, diffuse calcification, calcific degeneration and dystrophic calcification. It is defined as a pulpal response to trauma that is characterized by deposition of hard tissues within the root canal space.[1] Calcific metamorphosis occurs mainly due to traumatic injury of tooth, which can be detected early within 3 months; sometimes it cannot be detected even after 1 year. The tooth with traumatic injury usually results in partial or complete obliteration of the pulp canal and clinical crown discoloration. Other causes for calcific metamorphosis includes aging, systemic disease such as type 2 Dentinogenesis imperfect, orthodontic intrusion of tooth, irritants such as deep restorations and sometimes idiopathic.[2] Kronfeld and Boyle classified two types of pulp calcifications such as 1.Radicular pulp as diffuse (or) linear calcifications 2.Coronal pulp as denticles (pulp stones). Another calcification occurs most commonly by traumatic injury which ranges from 3.8 to 24%.[3] Generalized form occurs due to aging process of pulp. The exact mechanism of calcification is not clear. Several hypothetical theories have been proposed which varies from damaged neurovascular supply of pulp to formation of blood clot in the pulp canal leads to calcification.[4] It also suggests that following injury to apical vessels, if pulp remains vital instead of getting necrosed may leads to calcification.[5] The difficulty of managing such as calcified teeth requires sound knowledge about the anatomy and associated risks and complications. This case report explains the successful detection and management of calcified canal in the maxillary central incisor with the help of c+ files under microscope.
Case History
A 44-year-old male patient referred to department of endodontics with the chief complaint of pain and discoloured tooth in the upper front tooth region. Patient gave the history of trauma occurred 12 years ago in the upper front tooth region. He had no contributory medical history. On clinical examination, the right maxillary central incisor showed discoloration and presence of tender on percussion. Tooth showed negative response to thermal and electric pulp test. Periodontal probing depth and tooth mobility was within physiologic limit. On radiographic evaluations there is complete obliteration of pulp in 11 and widening of periodontal space around the root apex with bone loss in the distal aspect without any existing periapical pathology ([Figure 1]). Thus, provisional diagnosis of pulp necrosis with asymptomatic apical periodontitis was made and endodontic treatment was planned.
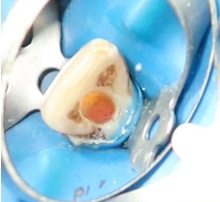
The proper assessment of tooth position and angulations was made and access cavity was initiated carefully after rubber dam isolation with the high speed no 4 round bur towards the pulp chamber in a stepwise removal of enamel and dentin. A proper access was made with the help of Endo Z bur under microscope. An endodontic explorer DG 16 was used to obtain catch point in the centre of tooth where tiny blackish discolouration point was noted. The line of patency of canal was negotiated with the help of no 8 c+ files, which is always maintained in the line parallel to the long axis of tooth. After reaching the middle third, the file inside the canal was verified with the radiograph. After checking the correct position of file in the canal, the working length was verified with another radiograph ([Figure 2]). A copious amount of 17% EDTA was used to demineralise the restricted hard tissues along the canal. The glide path was obtained using no 10 C+ files. Cleaning and shaping of canal done by rotary instruments till protaper F3. Irrigation was done with 5.25% NAOCL and normal saline in-between cleaning and shaping of all canals. After that calcium hydroxide dressing was done. Patient recalled after 2 weeks and obturation was done by protaper gutta percha with MTA Fillapex sealer ([Figure 3], [Figure 4], [Figure 5]). Finally, permanent restoration was done with composite restoration.






Discussion
The occurrence of calcific metamorphosis is more common in anterior teeth, but the exact mechanism of canal obliteration is unclear. The chance of pulp canal obliteration after dental trauma ranges from 4 to 24 %.[5] According to the American Association of Endodontics case assessment criteria, the endodontic treatment of the calcified teeth falls in high difficult treatment criteria. The first and foremost step in managing of calcified teeth requires proper knowledge about the anatomy of teeth, the clinical and radiographic evaluation and expertise clinical skills. After thorough diagnostic evaluation, initial step is the location of canal orifice using magnification. Dental Operating Microscope provides excellent magnification which results in precise identification of canal orifice in case of any calcification thus preventing procedural errors.[6], [7] This requires applying the law of root canal location, which states that pulp chamber always present in the centre of tooth at the level of CEJ, so the ideal location for access preparation is through incisal edge or nearer to that. The colour of pulp chamber which is darker than normal dentin also indicates the location of orifice. The bur must be entered with well centered direction along the long axis of teeth in an incremental removal of tooth structure up to the level of CEJ is necessary. The various diagnostic aids in locating canal orifice include methylene blue, champagne bubble test also useful in finding calcified canal. The next difficult part is negotiation and preparation of canal up to working length. Negotiation is done with the help of instruments such as endodontic explorer DG 16, canal pathfinder; C+ Files have the capacity to penetrate deeply inside the canal. The ideal file for negotiating calcified canal is C+ Files, because normal k files lacks rigidity and tends to fracture easily. C+ Files is more resistant to fracture and have 300% more resistant to buckling effect of normal k files.[8] Modified burs such as LN burs, Mueller bur helpful in negotiating calcified canals. Dental loupes, Dental operating microscope, CBCT, ultrasonic tips, Micro openers will increase the chance of negotiation and successful management of the calcified canal. Repeated assessment of the file path inside the canal should be checked with conventional radiographs is more important step in managing to avoid procedural errors. Once the working length is achieved always using crown down technique in preparing this canal is necessary, which increases the success of treatment and also reduces separation of instruments during instrumentation. The important step also includes the frequent use of chelating agents such as EDTA. It demineralizes the deeper hard tissues inside the canal and removes debris. It removes about 10.6 gms of calcium from 100 gms of calcium.[9] The use of liquid EDTA with a cotton pellet facilitates negotiation and lubrication of the calcified canal plays an important role in managing calcified canal. Endodontic microsurgery is the last option for managing calcified canals, where it is unable to locate the canal or endodontic treatment resulting in persistence of periapical pathology/symptoms.[10]
Conclusion
Thus, endodontic treatment of calcified canal is always challenging, because every step from diagnosis to obturation of canal poses some difficulty. Though negotiating and managing calcified canals can be challenging, they can be managed if a proper protocol is followed. The calcified canal should be managed properly by having knowledge about canal anatomy, Operator’s skill, patience and a proper armamentarium are the requisites to overcome the difficulties posed by these unforgiving canals for their successful treatment. This case is successfully managed by following proper access cavity preparation, following proper treatment guidelines, appropriate use of instruments for locating and negotiating the calcified canal which results in the success of root canal treatment.
Source of Funding
No financial support was received for the work within this manuscript.
Conflicts of Interest
There are no conflicts of interest.
References
- . Glossary of endodontic terms. 8th Edn.. American Association of Endodontists 2012. [Google Scholar]
- R Kronfeld, P E Boyle. Histopathology of the teeth and their surrounding structures. 4th Edn. 1955. [Google Scholar]
- FA Amir, JL Gutmann, DE Witherspoon. Calcific metamorphosis: A challenge in endodontic diagnosis and treatment. Quintessence Int 2001. [Google Scholar]
- S al-Nazhan, JO Andreasen, S al-Bawardi, S al-Rouq. Evaluation of the effect of delayed management of traumatized permanent teeth. J Endod 1995. [Google Scholar]
- PS McCabe, PMH Dummer. Pulp canal obliteration: an endodontic diagnosis and treatment challenge. Int Endod J 2012. [Google Scholar] [Crossref]
- P Krasner, HJ Rankow. Anatomy of the Pulp-Chamber Floor. J Endod 2004. [Google Scholar] [Crossref]
- B Thomas, M Chandak, A Patidar, B Deosarkar, H Kothari. Calcified Canals – A Review. IOSR J Dent Med Sci 2014. [Google Scholar] [Crossref]
- A Robertson. A retrospective evaluation of patients with uncomplicated crown fractures and luxation injuries. Endod and Dent Traumatol 1998. [Google Scholar] [Crossref]
- K Ajmera, S Mulay. Multimodality esthetic management - a case report. Int J Sci Res 2013. [Google Scholar]
- N Mittal, S Arora. Endodontic treatment of mandibular second premolar with three root canals using dental operating microscope. Endodontology 2009. [Google Scholar]